- Colorectal Cancer Is Rising among Younger Adults. Some States Want to Boost Awareness.
- Rural Hospitals Built During Baby Boom Now Face Baby Bust
- Food Stamps Go Further in Rural Areas — Until You Add Transportation Costs
- CMS Announces Resources and Flexibilities to Assist with the Public Health Emergency in the State of Texas
- CMS Proposes New Payments for Digital Health Under CY2025 PFS Draft Rule
- Improving Public Health by Strengthening Community Infrastructure
- Biden Harris Administration Proposes Policies to Reduce Maternal Mortality, Advance Health Equity, and Support Underserved Communities
- Nearly Half of U.S. Counties Don't Have a Single Cardiologist
- Randolph County, Ill. Turns Unused Part of Nursing Home Into State-Of-The-Art Behavioral Health Center
- Safe and Stable Housing Is a Foundation of Successful Recovery
- Rural RPM Program Is a Lifeline for Pregnant Women
- Expert: Rural Hospitals Are Particularly Vulnerable to Increasing Cyberattacks Targeting Healthcare Facilities
- Biden-Harris Administration Invests Over $200 Million to Help Primary Care Doctors, Nurses, and Other Health Care Providers Improve Care for Older Adults
- AJPH Call for Papers Special Section on Intersections of Public Health And Primary Care
- NIH HEAL Initiative Turns Attention to Pragmatic Trials in Rural Communities
Rural Pennsylvanians Have Nearby Access to Opioid Treatment, but Still Travel Far to Receive it

Rural Pennsylvania Medicaid enrollees diagnosed with opioid use disorder are driving an average of four times as far as their nearest prescriber to receive medication-assisted treatment, according to an analysis led by University of Pittsburgh Graduate School of Public Health researchers.
The study, published in the Journal of General Internal Medicine, also found that the farther people have to travel, the less likely they are to adhere to medication-assisted treatment, which is the standard of care for opioid use disorder.
 “While people in rural areas with opioid use disorder face challenges obtaining medication-assisted treatment, another important finding from our research is that these same people have substantial contact with their primary care physician, averaging four visits per year,” said lead author Dr. Evan Cole, research assistant professor in Pitt Public Health’s Department of Health Policy and Management. “By providing training and support to primary care physicians to provide medication-assisted treatment to their patients, policymakers might stimulate increases in treatment access in local communities.”
“While people in rural areas with opioid use disorder face challenges obtaining medication-assisted treatment, another important finding from our research is that these same people have substantial contact with their primary care physician, averaging four visits per year,” said lead author Dr. Evan Cole, research assistant professor in Pitt Public Health’s Department of Health Policy and Management. “By providing training and support to primary care physicians to provide medication-assisted treatment to their patients, policymakers might stimulate increases in treatment access in local communities.”
Medication-assisted treatment is the use of medications, such as buprenorphine, naltrexone or methadone, often with counseling, to treat opioid use disorder. The medications relieve opioid cravings and withdrawal symptoms. Providers must complete training and be approved to prescribe buprenorphine, and methadone can be dispensed only by licensed clinics for opioid use disorder.
Through a grant from the Agency for Healthcare Research & Quality to the Pennsylvania Department of Human Services, Cole and his colleagues reviewed Pennsylvania Medicaid claims data from 2014 to 2015 for 7,930 enrollees with a diagnosis of opioid use disorder living in 23 rural Pennsylvania counties heavily impacted by the opioid crisis. Pennsylvania is the seventh–largest Medicaid program by enrollment, the fourth–largest by expenditure and has the third–largest rural population, compared to other states.
The team mapped availability of providers of medication-assisted treatment and the actual location of where each enrollee was receiving treatment. The average distance to the nearest possible provider of medication-assisted treatment was 4.2 miles among rural enrollees with opioid use disorder. When the researchers limited it to only physicians with a high likelihood of taking new Medicaid recipients, the average distance was 12.6 miles. However, despite closer options, the Medicaid enrollees in the study were traveling an average of 48.8 miles for treatment.
“We can’t say for sure why the enrollees were traveling so much farther than necessary for treatment. We couldn’t measure things like wait times for appointments or patient preferences for particular providers,” Cole said. “But we do know that only 20 percent of those with opioid use disorder were diagnosed by their primary care physician. More frequently, they were diagnosed by a behavioral health provider, who then likely referred them to treatment.”
Getting someone with opioid use disorder into treatment is only the beginning, Cole said. His team took their analysis further and found that enrollees who travelled more than 45 miles to treatment had 29% lower odds of remaining adherent to medication-assisted treatment. There is strong evidence that adherence to medication-assisted treatment is related to a lower risk of relapse and improved outcomes.
“Primary care physicians don’t get a lot of training in addiction, so they may be reluctant to treat it due to concerns about administrative burdens on their practice or stigma about taking on new patients with opioid addiction,” Cole said. “But what we found is that the people in rural communities with opioid use disorder are already being seen by these primary care physicians for other reasons. If we can equip these physicians with training and administrative and clinical support to offer such treatment, and show them that they’ll be treating the patients they already have, they could be in the right place at the right time to address important gaps in access to addiction treatment.”
Cole said that future research will need to examine whether patients who are traveling great distances for medication-assisted treatment eventually switch to closer providers, and whether that change is associated with improved outcomes.
The research was funded by Agency for Healthcare Research & Quality grant 1R18HS025072-01. Ellen DiDomenico, M.S., of the Pennsylvania Department of Drug and Alcohol Programs is the principal investigator of the AHRQ grant, and is a co-author of the study.
Newly Released! Community HealthChoices (CHC) Toolkit
Through an Innovation Lab grant from the HealthSpark Foundation, the Pennsylvania Assistive Technology Foundation (PATF) collaborated with the Pennsylvania Health Law Project (PHLP) to create and disseminate a toolkit of materials that will help Pennsylvanians better understand Community HealthChoices (CHC). The toolkit, includes:
- CHC Infographic (English and Spanish)
- Person-Centered Service Planning
- How to Appeal a Denial in Community HealthChoices
- Where to Call for Help with Problems Consumers Experience in CHC – Southeast PA and Southwest PA
- Funding Your Assistive Technology: A Guide to Funding Resources in Pennsylvania (English and Spanish)
What is Community HealthChoices (CHC)?
CHC is a new waiver program for individuals over 21 years old with a disability who previously received services through the Independence, CommCare, or Aging Waivers. These individuals select or are automatically enrolled in one of three managed care organizations that have contracts with the state. Services are obtained through service providers who have contracts with these managed care organizations.
Services provided through CHC include all the Home and Community-Based Services formerly provided by waivers, plus a few new ones, for older adults and adults with physical disabilities or traumatic brain injury.
This program is in effect in 14 counties in Southwest Pennsylvania and 5 counties in Southeast Pennsylvania as of January 2019. The rest of the state will be covered in January 2020.
Pennsylvania Rural Hospital Leader Receives National Quality Spirit Award
University Park, Pa. (August 21, 2019) – Lannette Fetzer, quality improvement coordinator at the Pennsylvania Office of Rural Health (PORH), received the Medicare Beneficiary Quality Improvement Project (MBQIP) Spirit Award on July 11, 2019 at a national meeting in Bethesda, Maryland, convened by the Federal Office of Rural Health Policy (FORHP).
In 2011, FORHP, created MBQIP to promote high quality care at rural hospitals with 25 beds or fewer that have been designated at the federal level as Critical Access Hospitals (CAHs). Low-volume hospitals participating in the project voluntarily report on a set of quality measures relevant to the care they provide, share data and implement quality improvement initiatives. Currently, 98 percent of the 1,346 CAHs in the United States are reporting rural-relevant quality measures.
The nomination, submitted by Jennifer Edwards, rural health systems manager and deputy director at PORH, recognized Fetzer for being a rural health care leader and advocate since 1995 and for utilizing her extensive clinical experience to provide technical assistance in Pennsylvania and across the nation.
Edwards noted that Fetzer has worked diligently to ensure that the CAHs in Pennsylvania have the support they need to increase their quality metrics and expand quality improvement initiatives. Her efforts have yielded tremendous success as evident by Pennsylvania’s CAHs reporting rate of 100 percent for inpatient and outpatient MBQIP reporting measures. Since Fetzer joined PORH in 2016, Pennsylvania’s national ranking in the annual national recognition of state MBQIP programs has increased from fifth in 2017, to third in 2018 and now first in the nation for 2019.

“Lannette is passionate about rural health care,” said Edwards. “She has successfully partnered with the CAH quality improvement directors to improve patient outcomes across the Commonwealth. We are extremely proud of all her achievements.”
“This is an incredible honor for Lannette” noted Lisa Davis, director of PORH and outreach associate professor of health policy and administration at Penn State. “She is quickly emerging as a leader in the state and nationally for quality reporting and improvement in rural hospitals and health systems. Our office is proud to have Lannette as a member of our staff.”
Pennsylvania has 15 CAHs which serve the most rural communities in the state. Pennsylvania was one of the very first state to achieve 100 percent reporting by CAHs to MBQIP and is one of the few programs in the nation to have a staff member dedicated to quality improvement.
PORH formed in 1991 as a joint partnership between the federal government, the Commonwealth of Pennsylvania, and Penn State. The office is one of 50 state offices of rural health in the nation funded under a program administered by FORHP in the U.S. Department of Health and Human Services and is charged with being a source of coordination, technical assistance, and networking; and partnership development.
PORH provides expertise in the areas of rural health, agricultural health and safety, and community and economic development. PORH is administratively housed in the Department of Health Policy and Administration in the College of Health and Human Development at Penn State University Park.
Pennsylvania’s Critical Access Hospital Program Ranked Number One in the Nation for Quality Improvement
University Park, Pa. (August 22, 2019) – On July 11, at a national meeting in Bethesda, Maryland, the Federal Office of Rural Health Policy (FORHP) presented ten state offices of rural health with the 2019 Medicare Beneficiary Quality Improvement Project (MBQIP) Quality Performance Awards. These awards recognize achieving the highest reporting rates and levels of improvement in Critical Access Hospitals (CAHs) over the past year. CAHs are designated by the Centers for Medicare and Medicaid Services in recognition of the essential services they provide to rural communities.
This year’s 10 top-performing states are Pennsylvania, Massachusetts, Michigan, Utah, Alabama, Nebraska, Illinois, Maine, Minnesota and Wisconsin. These states’ offices of rural health built on their previous successes by investing funding from FORHP into quality-improvement projects and developing technical assistance resources that improve high-quality care in their communities. States also work collaboratively with each Critical Access Hospital and their respective partners to share best practices and utilize data to drive quality improvement in their hospitals.

Pennsylvania recently was ranked as the number one MBQIP program in the nation. The state has 15 CAHs which serve the most rural communities. Pennsylvania was one of the first states to achieve 100 percent reporting by CAHs to MBQIP and is one of the few programs in the nation to have a staff member dedicated to quality improvement.
The federally-funded program that provides technical assistance to the CAHs and supports their quality improvement efforts is administered by the Pennsylvania Office of Rural Health, which is administratively housed in the Department of Health Policy and Administration in the College of Health and Human Development at Penn State University Park.
Formed in 1991, PORH is one of 50 state offices of rural health in the nation funded under a program administered by FORHP. It is charged with being a source of coordination, technical assistance, networking, and partnership development, and provides expertise in the areas of rural health, agricultural health and safety, and community and economic development.
Lannette Johnston, quality improvement coordinator at PORH, said, “This award is evidence of the hard work and dedication that the Pennsylvania CAH quality improvement directors, staff and leadership provide every day to enhance the health of the communities they serve.”
“We are privileged to work with outstanding rural health care leaders who make quality care a top priority in their CAHs,” said Jennifer Edwards, PORH rural health systems manager and deputy director. “Receiving this recognition once again demonstrates their continued commitment to quality improvement.”
HRSA created the quality performance awards to promote high-quality care at rural hospitals with 25 or fewer beds. Hospitals that participate in MBQIP voluntarily report quality measures relevant to the care they provide, share data and take on quality improvement initiatives. Of those engaging in improvement initiatives, 72 percent have improved outcomes on the reported measures.
According to George Sigounas, HRSA administrator, “MBQIP is part of a broader portfolio of activities within HRSA to preserve hospitals and help rural communities to continue their access to quality health care. Ensuring rural hospital viability is an important component of HRSA’s strategic efforts on high-quality and value-based care.”
“We’re happy to work with the states on this effort,” said Tom Morris, FORHP associate administrator. “They’ve done a great job showing that CAHs can be national leaders in quality improvement and that results in better care in rural communities.”
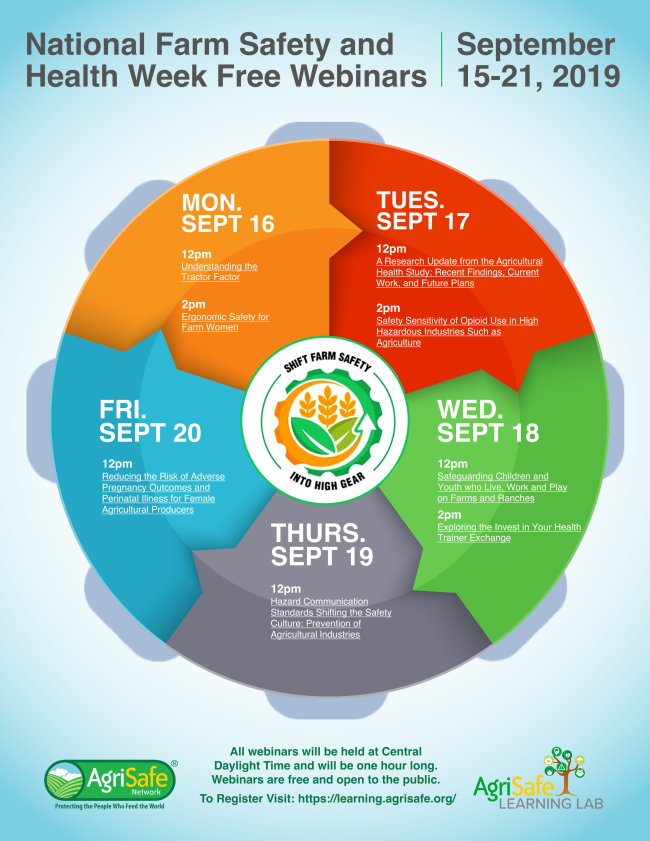
National Farm Safety and Health Week: September 15-21, 2019
AgriSafe Network is excited to be part of National Farm Safety and Health (NFSH) Week 2019. Participate in NFSH Week now by registering for FREE webinars relating to each of the daily topics! All you need to do to register is create a profile on the AgriSafe Learning Lab (which takes less than 2 minutes)! Google Chrome is the recommended web browser for the Learning Lab.
CLICK HERE to register and view a list of presenters!
The Candidates and Rural Policy: A Quick Guide
From The Daily Yonder
Here’s a roundup of the candidates’ positions on rural policy and a sampling of their statements about rural.
![]()
Eight of 19 Democratic presidential candidates have released comprehensive rural policy plans, and another six have included rural initiatives in other major policy documents, a Daily Yonder review of press reports and candidate websites reveals.
Only one candidate (New York Mayor Bill Deblasio) has been entirely mum on rural, according to our research. The other candidates have at least mentioned rural America on the hustings or in candidate debates. And most have created full rural plans or included rural implications in policy documents on topics such as economic development, healthcare, and conservation.
Candidates with comprehensive rural-policy platforms are former Vice President Joe Biden; South Bend, Indiana, Mayor Pete Buttigieg; former Ohio U.S. Representative John Delaney; New York Senator Kirsten Gillibrand; Colorado Governor John Hickenlooper; Minnesota Senator Amy Klobuchar; Vermont Senator Bernie Sanders; and Massachusetts Senator Elizabeth Warren.
Click here for a table of rural statements and documents from the 19 candidates who qualified for the second round of Democratic primary debates. The candidates are listed in alphabetical order. We’ll update this document as the campaign progresses. If you see errors or omissions, please let us know (tim@dailyyonder.com).
After A Rural Hospital Closes, Delays In Emergency Care Cost Patients Dearly
The loss of the longtime hospital in Fort Scott, Kan., forces trauma patients to deal with changing services and expectations.

Linda Findley’s husband, Robert, died after falling on the ice during a winter storm this February in Fort Scott, Kan. Mercy Hospital had recently closed, and Robert had to be flown to a neurology center 90 miles north in Kansas City, Mo., but at least three air ambulance pilots turned down the call from local EMS workers before one accepted.(Christopher Smith for KHN)
FORT SCOTT, Kan. — For more than 30 minutes, Robert Findley lay unconscious in the back of an ambulance next to Mercy Hospital Fort Scott on a frigid February morning with paramedics hand-pumping oxygen into his lungs. A helipad sat just across the icy parking lot from the hospital’s emergency department, which had recently shuttered its doors, like hundreds of rural hospitals nationwide.
Suspecting an intracerebral hemorrhage and knowing the ER was no longer functioning, the paramedics who had arrived at Findley’s home called for air transport before leaving. For definitive treatment, Findley would need to go to a neurology center located 90 miles north in Kansas City, Mo. The ambulance crew stabilized him as they waited.
But the dispatcher for Air Methods, a private air ambulance company, checked with at least four bases before finding a pilot to accept the flight, according to a 911 tape obtained by Kaiser Health News through a Kansas Open Records Act request.
“My Nevada crew is not available and my Parsons crew has declined,” the operator tells Fort Scott’s emergency line about a minute after taking the call. Then she says she will be “reaching out to” another crew. Nearly seven minutes passed before one was en route.
When Linda Findley sat at her kitchen counter in late May and listened to the 911 tape, she blinked hard: “I didn’t know that they could just refuse. … I don’t know what to say about that.” Both Mercy and Air Methods declined to comment on Findley’s case.
When Mercy Hospital Fort Scott closed at the end of 2018, hospital president Reta Baker had been “absolutely terrified” about the possibility of not having emergency care for a community where she had raised her children and grandchildren and served as chair of the local Chamber of Commerce. Now, just a week after the ER’s closure, her fears were being tested. Read the full article here.
Pennsylvania Governor Announces Double-Digit Decrease in State Overdose Rate
Pennsylvania Gov. Tom Wolf recently shared data that displays opioid overdoses have decreased in Pennsylvania by 18% from 2017 to 2018. Contributing to the decrease is the hard work and diligence of those working with patients who have a substance use disorder (SUD) to offer a combination of primary care services, medicated assisted treatment (MAT), recovery support specialists and individual and group therapy. The distribution of naloxone has also contributed to the decrease as has equipping first responders and other professionals with the opioid antagonist. The Wolf administration announced that two statewide naloxone distribution days will occur on Sept. 18 and Sept. 25 with details to be released in the next few weeks.
Rural Guide to Improving Chronic Obstructive Pulmonary Disease (COPD) Care
The National Rural Health Resource Center and Stroudwater Associates, supported by FORHP, developed a guide on the community and patient benefits for implementing pulmonary rehabilitation services. Rural hospitals and clinics can use this guide to identify areas for improvement within their diagnosis, treatment and long-term care of COPD patients in their communities. A University of Minnesota report highlights that while the COPD prevalence rate is the prevalence of COPD is higher for individuals living in rural areas, Critical Access Hospitals are less likely to employ any respiratory therapists. This guide is developed as part of the COPD National Action Plan, with the goal of developing resources for improving the lives of individuals living with COPD symptoms in rural communities. Click here to access the guide.
Rural Community Ambulance Agency Transformation Resource
This new resource helps rural emergency medical service leaders transform their agencies away from dependency on fees assessed for the volume of services provided and toward a people-centered, value-based operation that rewards positive patient outcomes. This resource was supported by the Federal Office of Rural Health Policy and coordinated by the Technical Assistance and Services Center (TASC), a program of the National Rural Health Resource Center. Click here to access the full document.